
Do you or someone you know play a sport? According to the National Survey of Children’s Health, over half of children and adolescents aged 6-17 years were involved in an organized sport such as soccer, basketball, or baseball in 2023, and this number continues to rise.
Youth sport participation can bring lots of benefits including physical fitness, teamwork, and discipline. However, young adults must also be careful, as their growing bodies put them at greater risk of injury than adults. Common sports injuries in children and adolescents include sprains and strains, overuse injuries, and concussions1Concussion: Brain injury caused by direct force to the head that can lead to the temporary loss of brain function. https://www.aans.org/patients/conditions-treatments/concussion/.

[Source: https://orthoinfo.aaos.org/globalassets/pdfs/know-the-signs-of-concussion_infographic_final.pdf]
A concussion is a type of brain injury caused by direct force on the head or a sudden change in speed or direction that negatively impacts brain function. The word “concussion” is derived from the Latin word “concusses,” meaning “to shake violently.” During a concussion, the brain moves back and forth inside the skull. This force causes the brain to release chemicals that make it harder for different regions of the brain to communicate with each other, resulting in concussion symptoms such as headaches, dizziness, memory issues, difficulty communicating, and lack of balance and coordination. Other symptoms of concussion may include confusion, nausea, sleepiness, irritability, and sensitivity to light.
Concussions can be difficult to diagnose because these brain changes do not often appear on imaging tests like a magnetic resonance imaging (MRI) or computed tomography (CT) scan. Instead, concussions are diagnosed based on an individual’s reported symptoms and a neurological exam2Neurological exam: Testing performed by a health care provider that checks the function of the brain, spinal cord, and nerves. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/neurological-exam that tests balance, coordination, and reflexes.

[Source: https://orthoinfo.aaos.org/en/diseases–conditions/sports-concussion/]
The best treatment for someone with a concussion is physical and mental rest. Tasks like reading, playing video games, or watching television can be taxing on the brain of someone with a concussion. Many children and adolescents with a concussion feel better within 2-4 weeks, but this timeline depends on multiple factors, including the severity of the concussion. Both the American Academy of Pediatrics and the American Academy of Neurology recommend that children and adolescents with a concussion be cleared by a health care provider before returning to play.
It is very important to make sure that you are fully healed from a concussion before jumping back into sports. This is because returning to activity too soon can lead to further injuries, including injury to the lower extremities (such as hips, knees, and feet) and repeat concussions. While a single concussion usually causes temporary effects that resolve with time, the effects of multiple concussions can be more long-lasting, including chronic headaches and challenges with concentration, memory, and balance. In addition, children and adolescents who have experienced multiple concussions are at greater risk for developing mental health problems and other chronic health issues.
It is important to note that scientific understanding of the specific causes of concussions as well as the potential consequences, especially in children and adolescents, remains poorly understood. Given the challenges of studying brain changes in humans over time, animal models play a critical role in improving our understanding of what happens during concussions and possible long-term outcomes. Animal models have made important contributions to our understanding of many types of traumatic brain injuries including concussions, and the development of animal models specific to sports-related concussions is already underway.
Developing a “Lab-in-a-box”
Taking time to fully heal after a concussion can be easier said than done. Dr. Jacob Thomas, postdoctoral research fellow at the University of Massachusetts, Amherst, is very familiar with wanting to get back in the game too soon, as a player and as a trainer. Dr. Thomas played high school football, where concussions forced him to the bench multiple times. “As an athlete, you just want to play no matter what,” he recalled. With other types of sports injuries, like a broken bone or muscle tear, physical pain can prevent an athlete from rejoining the game. However, concussions can be uniquely dangerous for motivated athletes because the player might still feel like they could keep going, despite their injury.
As an undergraduate, Dr. Thomas studied to become an athletic trainer, where he saw concussions from a different perspective. “As a trainer, it’s your job to help diagnose a concussion and determine whether it’s safe for an athlete to play—no matter what they tell you,” he recalled.
It was in his role as an athletic training student that Dr. Thomas started to notice the challenges with currently available methods for diagnosing concussions. The most common diagnostic tool for concussions used by both health care professionals and athletic trainers is called the Sport Concussion Assessment Tool 6, or SCAT6. The SCAT6 is appropriate for adolescents aged 13 years and older. For children aged 8 to 12 years, the tool has been adapted and is called the Child SCAT6.
The SCAT6 has multiple sections including symptoms reported by the athlete and more objective measures of memory, coordination, and balance. This means that symptoms reported by the athlete such as dizziness, nausea, vision problems, and headaches impact how the tool assesses the presence or absence of a concussion. For athletes who really want to continue the game, they can underreport symptoms to make it more likely they will be cleared to play.
In his graduate work, Dr. Thomas sought to develop a new tool that would include only objective measurements without relying on symptoms reported by affected players. The tool needed to be inexpensive to be easily incorporated into athletic training departments and small enough to be used on site or game-side.
Dr. Thomas started this project with large, expensive equipment that can only be found in a biomechanics3Biomechanics: The study of how physics and forces apply to the movement of living organisms. https://biomechanicseducation.com/what-is-biomechanics-biomechanics-education/ laboratory, such as the Mizzou Motion Analysis Center (MAC) where this work was completed. This equipment allows Dr. Thomas and other researchers to capture the precise movements and forces at play while a participant walks, runs, or performs other activities. For example, participants wear reflective markers on different points of their body that connect to a camera system that captures motion from different angles. On the ground, force plates measure the amount and direction of forces as participants move.

[Source: Mizzou Motion Analysis Center]
While this might be the gold standard for assessing the coordination and balance of an athlete with a suspected concussion, this kind of equipment is only available in academic research centers and cannot practically be used by athletic trainers in the moment. Instead, Dr. Thomas hoped to create a “lab-in-a-box,” that could take similarly precise measurements but with technology that is more inexpensive and easily available. The lab-in-a-box that he developed included three components:
- The XBox Azure Kinect camera to capture motion. This is a low-cost camera that creates a projection of a skeleton on the screen and provides some information about where an individual is in space without wearable reflective markers. This is the type of camera used in the video game Dance Dance Revolution (DDR), released in the late 1990s.
- Force plates created by Dr. Thomas and the MAC lab team. Dr. Thomas describes these force plates as “glorified bathroom scales.” Together, the camera and force plates show where the feet are pushing (measured by the force plate) and where the body is in space (measured by the camera). These measurements show how well an individual can coordinate and balance while doing specific tasks.
- A reaction time board (also called an interface board) using a system of lights and buttons to measure reaction time, a key metric for diagnosing a concussion. This system allowed the researchers and anyone using the tool to determine whether a participant’s reaction time (the time between when the light turns on and when the participant presses the button) was delayed. Dr. Thomas and the MAC team developed this reaction time board in the laboratory.
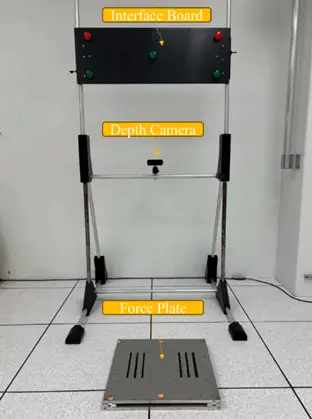
[Source: Thomas et al 2025, Fig 1]
With all the components of the lab-in-a-box optimized, the next step was to validate this tool against the gold standard equipment in the research laboratory. Dr. Thomas invited athletes who had recently experienced a concussion to participate in a research study comparing the two sets of equipment.

[Source: Thomas et al 2025, Fig 2]
The results showed that the lab-in-a-box equipment worked just as well as the gold standard laboratory equipment at taking the measurements needed to assess the presence of a concussion. The tool was called the Mizzou Point-of-Care Assessment System, or MPASS for short.
Figure 6: The Mizzou Point-of-Care Assessment System
[Source: https://mizzoumotioncenter.com/MPASS_Athletic.html ]
Bringing MPASS to the Game
It was now time to test the lab-in-a-box in a real-world setting. To make this happen, Dr. Thomas approached athletic trainers at nearby universities in Missouri whose athletic programs were part of the National Association of Intercollegiate Athletics. When an athlete was diagnosed with a concussion, the athletic trainer would invite the athlete to participate in Dr. Thomas’s research study.
A total of 20 athletes who experienced a concussion agreed to participate in this research. The athletes played a variety of sports including soccer, cheerleading, football, track, and softball. Dr. Thomas invited an additional 20 athletes who did not experience a concussion in the past year to participate as the control group. These athletes were matched by sport and position to the athletes who experienced a concussion. For example, if a cheerleader whose position was base had a concussion, another base cheerleader who had not experienced a concussion was invited to participate as a control.
Dr. Thomas analyzed the collected data using an explainable machine learning algorithm4Machine learning algorithm: Instructions that enable computers to learn from a data set and use data to make predictions and improve over time. https://www.geeksforgeeks.org/machine-learning/machine-learning-algorithms/. Machine learning is a type of artificial intelligence that uses algorithms to find patterns in data and make decisions. In this case, Dr. Thomas needed the algorithm to take all the measurements collected from the lab-in-a-box and make a binary decision: does this athlete have a concussion, or not?
First, Dr. Thomas entered half of the data into the algorithm for training purposes. Dr. Thomas tuned the algorithm so that it could correctly assess whether an individual had a concussion or not based on the given data. Once the algorithm had been calibrated, Dr. Thomas tested the algorithm on the other half of the data that it had never seen before.
Based on metrics gathered from the lab-in-a-box, the machine learning algorithm was 82.5% accurate. If an individual had a concussion, the algorithm could correctly identify the presence of a concussion 75% of the time. If an individual did not have a concussion, the algorithm could correctly identify the absence of a concussion 90% of the time. “These numbers are far better than what we have seen with other predictive models developed by other researchers,” remarked Dr. Thomas. “We were very happy with these results.”
Because this machine learning algorithm was explainable, Dr. Thomas and colleagues could see which of the input measurements the algorithm used to come to a decision. “The algorithm used all the different measurements we gave it, which is a really good sign,” added Dr. Thomas. “The purpose of the machine learning model is to take many different metrics and come up with an answer, and the results showed that the algorithm did just that.” This is a great example of how technology can move medical innovation forward.
Moving Forward
While these results are promising, this is not the final model. Dr. Thomas would like to see ongoing testing to improve the model and make sure it is as accurate as possible under different settings. For example, the study methods could be improved by testing all participating athletes at the beginning of the season, and then again if they experience a concussion. Since the impacts of a concussion can be so variable among individuals, this would allow for more fine-tuning of the measurements.
In addition, Dr. Thomas would like to see researchers provide ongoing follow-up for participants as they recover. Trying to recover from an injury can be particularly challenging if an individual cannot sense or feel that they’re making progress. By employing this tool multiple times over the course of recovery, athletes would be able to track their progress and compare their results. In addition, the model might be able to show physical therapists and other rehabilitation specialists areas of particular weakness to focus on for a specific individual. This is known as precision rehabilitation.
As for Dr. Thomas, since graduating with his PhD, he continues to work with the same biomechanical tools to solve a different problem: assessing the biomechanical components of fatigue in older adults to understand why they get more tired as they age and how that might affect mobility.
Dr. Jacob Thomas is a postdoctoral research fellow in the Biomechanics Lab and Musculoskeletal and Orthopedic Biomechanics Lab Group run by Dr. Katherine Boyer at the University of Massachusetts, Amherst. He completed his PhD at the University of Missouri where he was involved in the development of the Mizzou Point-of-care Assessment System (MPASS), described here. When not in the laboratory, Dr. Thomas enjoys running, playing guitar, tinkering with electronics, and spending time with his family.
- Thomas JM, Hall JB, Bliss R, Leary E, Sayers SP, Rao P, Guess TM. A machine learning approach to concussive group classification using discrete outcome measures from a low-cost movement-based assessment system. Med Eng Phys. 2025 Oct;144:104402. https://iopscience.iop.org/article/10.1016/j.medengphy.2025.104402
- Mizzou Motion Analysis Center. https://mizzoumotioncenter.com/technologies.html
- Sport Concussion Assessment Tool 6. https://bjsm.bmj.com/content/bjsports/57/11/622.full.pdf
- Child SCAT6. https://bjsm.bmj.com/content/bjsports/57/11/636.full.pdf
- American Academy of Pediatrics. https://www.healthychildren.org/English/health-issues/injuries-emergencies/sports-injuries/Pages/Concussions.aspx
- American Academy of Orthopedic Surgeons. https://orthoinfo.aaos.org/en/diseases--conditions/sports-concussion/
- Centers for Disease Control and Prevention. https://www.cdc.gov/heads-up/about/index.html
- A Neurologist's Step-by-Step Guide to Concussion Recovery. https://www.neurahealth.co/blog/a-neurologists-step-by-step-guide-to-concussion-recovery
- Written by Rebecca Kranz with Andrea Gwosdow, PhD at http://www.gwosdow.com

